Novartis AG and Others (Claimants/Appellants) v Focus Pharmaceuticals UK Ltd and Others
| Jurisdiction | England & Wales |
| Judge | Lord Justice Kitchin,Lord Justice Floyd,Lord Justice Hamblen |
| Judgment Date | 21 December 2016 |
| Neutral Citation | [2016] EWCA Civ 1295 |
| Court | Court of Appeal (Civil Division) |
| Date | 21 December 2016 |
| Docket Number | Case No: A3/2015/2032 & 2033 |
[2016] EWCA Civ 1295
IN THE COURT OF APPEAL (CIVIL DIVISION)
ON APPEAL FROM THE HIGH COURT OF JUSTICE
CHANCERY DIVISION (PATENTS COURT)
THE HON MR JUSTICE ARNOLD
Royal Courts of Justice
Strand, London, WC2A 2LL
Lord Justice Kitchin
Lord Justice Floyd
and
Lord Justice Hamblen
Case No: A3/2015/2032 & 2033
Thomas Hinchliffe QC (instructed by Bristows LLP) appeared for the Claimants/Appellants
Daniel Alexander QC and Henry Ward (instructed by Olswang LLP) appeared for Focus Pharmaceuticals Ltd
Daniel Alexander QC and Henry Ward (instructed by Pinsent Masons LLP) appeared for Actavis
Daniel Alexander QC and Mark Chacksfield (instructed by Bird & Bird LLP) appeared for TEVA UK Ltd
Hearing dates: 1 st and 2 nd November 2016
Approved Judgment
Introduction
In these actions the claimants (together "Novartis") alleged that the defendants ("Focus" and "Actavis" in action HP-2013–000011 and "Teva" in action HP-2013–000012) had infringed European Patent (UK) No. 2,292,219 entitled "Transdermal therapeutic system for the administration of rivastigmine" ("the Patent"). The Patent has a single EPC 2000 claim which is directed to rivastigmine for use in a method of preventing, treating or delaying the progression of Alzheimer's disease ("AD") in which the rivastigmine is administered in a transdermal therapeutic system ("TTS"), that is to say a patch, at a particular starting dose. The defendants denied infringement and counterclaimed for revocation of the Patent on the grounds of added matter, obviousness and insufficiency.
The action came on for trial before Arnold J in March 2015. In his judgment, handed down on 27 April 2015 [2015] EWHC 1068 (Pat), he found that the Patent lacked any inventive step over a single piece of prior art, US Patent No. 6,335,031 ("US 031"), and was also invalid for added matter. He rejected the allegation of insufficiency. He also held that if the Patent had been valid, the defendants would have infringed it.
Novartis now appeals against the judge's order revoking the Patent. Originally the defendants all supported the judge's conclusions in relation to obviousness and added matter but contended that he fell into error in construing the claim and that, if he had construed it properly, he would have found that none of their activities fell within its scope. They also contended that if the Patent was not obvious, it was insufficient. However, at the outset of the appeal we were informed that Novartis and Teva had resolved their differences and agreed a compromise of the claim and counterclaim in action HP-2013–000012. Accordingly, we proceeded to hear the appeal in action HP-2013–000011 against Focus and Actavis. We have now been informed that Novartis has also agreed confidential terms of settlement with Actavis and Focus as a result of which Novartis' claim for infringement has been compromised. However, Novartis maintains its appeal against the order for revocation.
There are two other matters I must mention at the outset. First, the Patent has been opposed before the European Patent Office by, at least originally, 13 opponents. The oral proceedings before the Opposition Division took place on 15 December 2015 and for reasons set out in a decision dated 15 March 2016, it decided that the Patent must be revoked for added matter. Its order for revocation has been suspended pending appeal. Secondly, other designations of the Patent and equivalent national rights have been extensively litigated in proceedings in other jurisdictions. As the judge noted, there has been a striking diversity of outcomes, with some courts and tribunals finding infringement and others not. Until the decision of the judge, there had been no final decision on validity, however.
I will address each of the issues which remain to be decided upon this appeal but first must say a little about the technical background and describe the relevant disclosure of the application for the Patent and of the Patent itself.
The technical background
The judge addressed the technical background from [11] to [33] of his judgment. The following points are material to this appeal.
AD is a progressive neurodegenerative disease that causes dementia and, ultimately, death. One of the key underlying mechanisms of the cognitive dysfunction associated with AD is a loss of the neurotransmitter acetylcholine ("ACh") in the brain. ACh is synthesised within presynaptic cells and, once released, interacts with receptors on postsynaptic cells. The activation of these postsynaptic receptors leads to the propagation of nerve impulses.
ACh is quickly inactivated by an enzyme called acetylcholinesterase ("AChE"). One way of addressing the cholinergic deficit associated with AD is therefore to inhibit AChE. Such inhibition leads to increased levels of ACh as the rate of its breakdown is attenuated.
Three AChE inhibitors were commonly used for the treatment of mild to moderate AD at the priority date, namely donepezil, galantamine and rivastigmine. All were administered orally and all were associated with mild to moderate cholinergic side effects such as nausea, vomiting and diarrhoea. These side effects were managed by titrating the dose administered to patients gradually upwards as their tolerance increased. However, that tolerance was quickly lost if treatment was interrupted for more than a few days.
At the priority date, donepezil was the UK market leader and galantamine and rivastigmine were generally considered to be second line treatments. Importantly, donepezil was perceived to have a number of significant advantages over rivastigmine: it only required a single daily dose, rather than twice daily doses, resulting in higher patient compliance and carer convenience; administration began with a clinically effective dose, whereas the initial dose of rivastigmine was sub-therapeutic; it had a less complicated treatment regime than rivastigmine; and it was perceived to have less severe side effects than rivastigmine.
Rivastigmine was sold under the brand name Exelon and was formulated in capsule and oral solution form. Treatment began with the administration of 1.5 mg twice daily (bis in diem or "b.i.d."). At intervals of between two and four weeks, the dose was increased in steps of 1.5 mg up to a dose of 6 mg b.i.d. The minimum effective dose was 3 mg b.i.d.
Various parameters are used to assess the pharmacokinetic properties of an active pharmaceutical ingredient ("API") such as rivastigmine, namely:
i) "C max" which is a measure of the peak plasma concentration of the API;
ii) "t max" which is the time at which C max is reached; and
iii) "AUC" or "area under the curve" which, as its name suggests, is the area under the concentration-time curve and reflects the exposure of the body to an API after administration. AUC24h is the AUC over a 24 hour period.
The Summary of Product Characteristics ("SmPC") for Exelon capsules explained how they should be administered, gave warnings and precautions for use and detailed the drug's pharmacodynamic properties. It explained that rivastigmine should be administered b.i.d., with morning and evening meals, and that administration in this way delayed absorption assessed by reference to t max by 90 minutes, lowered C max and increased the AUC by approximately 30%.
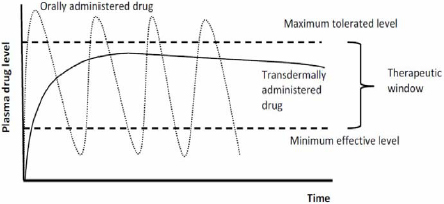
A TTS is applied to the skin to deliver the API it contains into the bloodstream. There were, at the priority date, no available TTSs for the treatment of AD. Nevertheless, it was known that transdermal administration had a number of advantages over oral administration including the provision of a smoother delivery curve, so avoiding the rapid fluctuation and peak levels of drug plasma concentration often seen with APIs administered orally. Professor Williams, the defendants' expert witness in the area of transdermal formulation, illustrated this effect in this way in his first report:
Nevertheless, it was also understood that administration by transdermal means had the various disadvantages identified by the judge at [27]:
i) only a limited number of APIs are suitable for administration in this way;
ii) TTSs are generally more expensive and time consuming to develop than oral formulations;
iii) the onset of treatment tends to be slower than with oral formulations; and
iv) there is the potential for local skin irritation.
It was also known to be desirable to provide patients with a fixed and reproducible dose of the API over the prescribed period of application and that for this reason the rate of release should be constant. In the case of administration by TTS, this was achieved by ensuring that, so far as possible, the TTS was saturated with the API for the entire period of application.
The development of a TTS would begin with the provision by the clinician to the formulator of a target dose. The judge explained how matters progressed thereafter in these terms with which neither side took issue:
"31. Once an API is identified as being suitable for delivery by a patch, a target dose would be given to the formulator by the clinician and would generally be quantified in terms of a target AUC, typically the AUC24h. The target AUC24h will normally correspond to the AUC24h for the oral dosage form.
32. Once the target dosage is selected, prototypes will be produced and tested in short term accelerated and real time stability tests and their...
To continue reading
Request your trial
-
UK Supreme Court Explains The Law Of Obviousness
...failed to confer inventive step in Generics v Yeda [2017] EWHC 2629 (Pat), FKB v AbbVie [2017] EWHC 395 (Pat), Novartis v Focus [2016] EWCA Civ 1295, Hospira v Cubist [2016] EWHC 1285 (Pat), Richter v Generics [2016] EWCA Civ 410, Accord v medac [2016] EWHC 24 (Pat) and Hospira v Genentech ......