Rebeccah Taylor v Chesterfield Royal Hospital NHS Foundation Trust
| Jurisdiction | England & Wales |
| Judge | John Kimbell |
| Judgment Date | 30 April 2019 |
| Neutral Citation | [2019] EWHC 1048 (QB) |
| Court | Queen's Bench Division |
| Date | 30 April 2019 |
| Docket Number | Case No: HQ16C03583 |
[2019] EWHC 1048 (QB)
IN THE HIGH COURT OF JUSTICE
QUEEN'S BENCH DIVISION
Royal Courts of Justice
Strand, London, WC2A 2LL
John Kimbell QC
(sitting as a Deputy High Court Judge)
Case No: HQ16C03583
Christopher Kemp (instructed by Tozers LLP) for the Claimant
Farrah D. Mauladad (instructed by Weightmans LLP) for the Defendant
Hearing dates: 4, 5, 6 and 7 February 2019
APPROVED JUDGMENT
I direct that pursuant to CPR PD 39A para 6.1 no official shorthand not shall be taken of this Judgment and that copies of this version as handed down may be treated as authentic.
John Kimbell QC sitting as Deputy High Court Judge:
INTRODUCTION
The Claimant is 26 years old. She was born at Royal Chesterfield Hospital (‘ the Hospital’) on 13 November 1992. On that day she suffered a brachial plexus injury which she alleges was the result of negligence on the part of the two midwives and/or the registrar who attended her birth.
The brachial plexus is a network of nerves which emerge from the neck region of the spine. It conducts signals from the brain to the muscles of the shoulder and forearm. If these nerves are stretched beyond a certain point, they can rupture. If the damage is significant, it can lead to a permanent paralysis of the arm usually referred to as Erb's (or Erb-Duchenne) palsy.
The Claimant is the second of four children. Her older brother, Oliver, was born in December 1990. Her younger brother, Harry, followed in October 1995 and younger sister, Holly, in 1999. Her parents are Deborah Taylor and Christopher Taylor. They are clearly a close, supportive and loving family.
Rebeccah was delivered at 20:35 by Dr Dobbs, a registrar. He had been summoned by the two midwives who had been in attendance up that point, Mrs Julie Rawson and Student Midwife Godfrey. They summoned Dr Dobbs because the delivery of Rebeccah's body had not followed the delivery of her head in the usual way, i.e. with the next contraction. The reason for the interruption in delivery was that Rebeccah's anterior (left) shoulder had become lodged underneath her mother's pubic bone in a condition referred to as shoulder dystocia.
The entry in the agreed delivery notes signed by Dr Dobbs states:
“SHOULDER DYSTOCIA – [head] delivered
episiotomy cut + ant. shoulder del.
[with] suprapubic pressure + traction”.
It was noted immediately after her birth that Rebeccah's left arm was floppy. It was thought that she might have suffered a fractured clavicle. An x-ray revealed that there was in fact no fracture but Rebeccah was subsequently diagnosed as having a Group 2 obstetric brachial plexus injury (‘ OPBI’). The categorisation referred to is that developed by Gilbert and Tassin and described by Narakas in the table below: 1
| Group | Roots injured | Site of weakness / paralysis | Likely Outcome |
| 1 | C5, C6 | Shoulder abduction/external rotation, elbow flexion | Good spontaneous recovery in over 80% of cases |
| 2 | C5, C6, C7 | As above but with drop wrist | Good spontaneous recovery in about 60% of cases |
| 3 | C5, C6, C7, C8, T1 | The whole plexus has been damaged. Complete flaccid paralysis | Recovery in 30%-50% of cases |
| 4 | C5, C6, C7, C8, T1 | Complete flaccid paralysis with Horner Syndrome | Without surgery severe defects throughout the limb. Full spontaneous recovery never occurs |
In Rebeccah's case a spontaneous recovery has not occurred. She has not undergone any surgery and the loss of range of movement in her left arm is significant. This affects her daily life in a number of ways. She suffers back and shoulder pain. Notwithstanding all the challenges presented by her birth injury, she has thrived. She achieved bronze, silver and gold swimming medals at school and participated fully in dance and PE lessons as well as skiing trips. She took A-levels and obtained a graphic design degree from Manchester University. She has travelled and worked abroad.
Rebeccah's parents did not bring a claim against the Hospital on her behalf while she was a child. However, whilst at university, Rebeccah began to research her birth injury and in 2013 she obtained a legal aid certificate to pay for legal advice. A letter of claim followed in July 2014 and a claim form was issued on 17 October 2016.
No limitation defence was pleaded by the Defendant.
THE PLEADED CASE
In summary, the Claimant alleges that her brachial plexus injury was caused by the negligent application of excessive traction to her head by the attending midwives and/or the registrar after shoulder dystocia had been correctly diagnosed by the midwives. The Defendant denies liability on the basis that the procedures in place and the steps taken in response to Rebeccah's shoulder dystocia were in accordance with practices accepted as proper by a responsible body of medical people in 1992.
There were originally six pleaded breaches of duty, namely:
(a) Attempting to apply suprapubic pressure while Mrs Taylor remained in the left lateral position.
(b) Failing to move Mrs Taylor into the dorsal position before applying suprapubic pressure.
(c) Failing to alter the maternal position after the attempt to deliver in the left lateral position as a manoeuvre to overcome the shoulder dystocia.
(d) Either by the midwives or Dr Dobbs applying excessive traction to the Claimant's head in an attempt to deliver her shoulders.
(e) Either by the midwives or Dr Dobbs applying more than diagnostic traction to the Claimant's head in an attempt to deliver her shoulders.
(f) Either by the midwives or Dr Dobbs applying traction to the Claimant's head such as to damage permanently her (left) brachial plexus.
However, in the course of the trial, the first three allegations set out above were abandoned. The case thus becomes a case about traction.
QUANTUM
Quantum was agreed in the sum of £1,150,000.
MEDICAL FACTUAL BACKGROUND
Mrs Taylor's due date was 2 November 1992. On 8 November 1992, Mrs Taylor was admitted to the Hospital's Labour Suite with a suspected spontaneous rupture of membranes and occasional uterine tightening. Following a medical review, Mrs Taylor was allowed to go home with an antenatal clinic appointment.
On 12 November 1992, Mrs Taylor attended her final antenatal assessment. By now, she was 10 days past her due date. It was noted that Rebeccah was a “big baby”. A vaginal examination was performed and Mrs Taylor's cervix was found to be 2cm dilated. It was noted that Mrs Taylor was “anxious” and had requested induction of labour. Mrs Taylor was admitted at 18.40. The admitting midwife noted that Mrs Taylor had “anxiety re size of baby & method of induction”.
Mrs Taylor was assessed at 06.00 on 13 November. She had slept very little overnight because of discomfort. On vaginal examination her cervix was slightly posterior but fully effaced and 3–4cm dilated. The baby's head was presenting. Mrs Taylor was transferred to the Hospital's Central Delivery Suite at 08.00.
At 10.30 a vaginal examination was carried out to rupture the membranes. The cervix was 4cm dilated. Clear liquor was draining but Mrs Taylor was only contracting irregularly.
At 13.45 Mrs Taylor's contractions were recorded as being irregular and mild to moderate only. Therefore, a plan was made to commence the use of syntocinon to stimulate uterine activity.
At 14.00 Mrs Taylor's care was taken over by student midwife Godfrey and Mrs Rawson.
At 14.45 a syntocinon infusion was started.
At 17.40 a vaginal examination was performed. Mrs Taylor's cervix was found to be 6cm dilated and the forewaters were found to be intact. These were ruptured, releasing clear fluid. The lack of progress of cervical dilatation was noted, with a plan to reassess in two hours. The foetal heart showed a good trace.
At 19.30 Mrs Taylor is recorded as saying that she was feeling “pushy”. The partogram records strong contractions every 2 minutes at this point.
At 20.00 a vaginal examination was performed. The cervix was fully dilated with strong contractions every 2 minutes.
At 20.10 active pushing is recorded as having commenced.
At 20.30 an entry made by student midwife Godfrey recorded the “controlled delivery of head”. The timing of this entry was subsequently changed to “20.32 approx” by Mrs Rawson. The explanation for this change was explored in cross-examination.
Rebeccah was born at 20.35. She weighed 4.93 Kgs (10 lb 14 oz). Mrs Taylor needed 40 stiches to repair extensive second-degree tears.
What happened between the delivery of Rebeccah's head at 20.30 (or approximately 20.32) and the rest of her body between 3 and 5 mins later is in dispute.
Mrs Rawson's note
A significant portion of the trial was spent exploring the following note in the Medical Records made by Mrs Rawson:
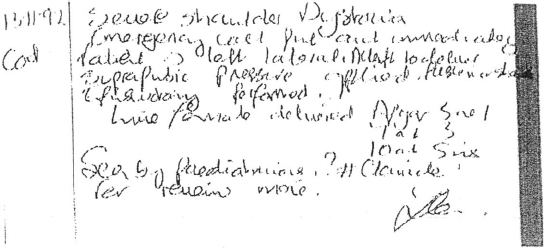
In her evidence Mrs Rawson said she thought she would have written this note at the end of her shift (at around 21.00) on 13 November 1992. I accept that evidence. It was eventually agreed that this note was to be read as follows with numbers in [ ] to indicate line numbers.
[1] Severe shoulder Dystocia
[2] Emergency call put out immediately
[3] Patient → left lateral. Attempt to deliver posterior shoulder
[4] Suprapubic pressure applied
[5] Episiotomy performed.
[6] Live female delivered Apgar 5 at 1
[7] 7 at 3
[8] I O at 5 mins.
[9] Seen by paediatricians. ?[fracture] clavicle
[10] for review mane.
[Signature of Mrs Rawson]
There was originally a dispute about when the words “ Attempt to deliver posterior shoulder” were added. However, Mrs Rawson explained in evidence, and it was accepted by Mr Kemp on behalf of the Claimant in his closing submissions, that these words were added at the same time as the rest of the...
To continue reading
Request your trial
-
Mrs Matilda Clarke (in her personal capacity and as executor of the estate of Mr Lloyd George Clarke deceased) (a protected party by her litigation friend Mrs Elizabeth Shirley St Hill) v Ms Vinette Dawn Allen
...April 2019, Mr John Kimbell QC sitting as a High Court Judge handed down judgment in Taylor v Chesterfield Royal Hospital NHS Trust [2019] EWHC 1048 (QB). I have not referred it to Mr Ng as the principles are uncontroversial. Mr John Kimbell QC said at paragraph 112 “It is not appropriate ......